An atypical presentation of polymorphic eruption in early pregnancy in a 40-year-old female: case in images
SPMC J Health Care Serv. 2023;9(2):2 ARK: https://n2t.net/ark:/76951/jhcs48xse6
1Department of Dermatology, Southern Philippines Medical Center, JP Laurel Ave, Davao City, Philippines
Correspondence Andrea Isabel Contreras, andiscontreras@gmail.com
Received 12 May 2022
Accepted 5 October 2023
Cite as Contreras AI, Belisario MP. An atypical presentation of polymorphic eruption in early pregnancy in a 40-year-old female: case in images. SPMC J Health Care Serv. 2023;9(2):2. https://n2t.net/ark:/76951/jhcs48xse6
Polymorphic eruption in pregnancy (PEP), formerly known as pruritic urticarial papules and plaques of pregnancy, is a common gestational dermatosis. It rarely manifests in the early trimester of pregnancy and hardly persists in the postpartum period especially in multigravid patients. PEP usually appears late in the third trimester of a first pregnancy, and less frequently in the immediate postpartum period. It occurs almost exclusively in primigravid mothers and is more common in multiple pregnancies.1 2 3 Recurrence in subsequent pregnancies is extremely rare.3 4 The cause of PEP is still unknown, although various theories have been proposed, including increased skin distention, deposition of fetal DNA in skin lesions, high levels of progesterone, and increased progesterone receptor immunoreactivity in patients with PEP.3 5 6
PEP usually presents with pruritic, erythematous papules and plaques on the trunk and extremities, occasionally accompanied by vesicles and bullae. The condition spares the umbilical and facial regions, and lesions initially appear on areas with striae. There are no mucosal lesions associated with this condition.3 5
The diagnosis of PEP is primarily clinical, relying on the patient’s history and physical examination (PE). Skin biopsy may be useful to rule out other potentially aggressive skin eruptions in pregnancy, such as pemphigoid gestationis (PG), which can mimic PEP in the early urticarial phases.5 7 However, in contrast to PEP, PG typically begins in the second to third trimester of pregnancy, predominantly affecting multiparous patients, and carrying potential risks to the fetus.8 Differentiating PEP from other conditions with similar presentations, such as drug reactions, scabies, and viral syndromes, necessitates a comprehensive evaluation involving clinical history, histology, and serology.2 5 The prognosis of PEP is excellent, with spontaneous resolution of symptoms within a few weeks after delivery. It also does not pose an increased risk of maternal or fetal morbidity.7
We present the case of a 40-year-old female who developed erythematous vesicles on her face during the first trimester of her second pregnancy. The lesions gradually spread to other areas of the body and persisted until two weeks postpartum, then they spontaneously resolved. However, the lesions intermittently reappeared several months postpartum.
A 40-year-old female, gravida 2 para 2, with two living children from two previous full term deliveries, presented at our clinic at 26 weeks postpartum, with a history of more than one year of generalized vesicles and urticarial plaques. The lesions started when the patient was in the fourth week of gestation of her second pregnancy. She developed multiple erythematous vesicles on her chin, associated with pruritus that was aggravated by heat and perspiration. In the eighth week of gestation, the patient had erythematous plaques on her neck and chest, which prompted her to seek consultation with a dermatologist who did not prescribe any oral or topical medications due to her pregnant condition. The vesicular lesions, which ranged from 3 to 5 centimeters in diameter, contained clear serous fluid, and they gradually spread to the abdomen and the bilateral upper and lower extremities. At this time, she applied coconut oil to her affected body parts. She developed hyperpigmentation after the vesicles ruptured and healed, and she was then able to give birth via Cesarean section without any complications.
At two weeks postpartum, there was complete resolution of all symptoms with consequent hyperpigmentation. At six weeks postpartum, there was gradual recurrence of lesions in the previously involved areas. This prompted the patient to consult another dermatologist, who prescribed oral prednisone for her at a dose of 1 mg per kg per day tapered down over a month. This resulted in the resolution of all blisters and erythematous plaques. At 18 weeks postpartum, however, there was recurrence of lesions on the upper chest, which prompted the patient to self-medicate intermittently with oral prednisone at 20 mg twice or thrice daily, with partial resolution of symptoms. As a result, at 26 weeks postpartum, the patient finally decided to seek further consultation at our clinic.
The patient did not report any fever or associated symptoms, and her umbilicus, palms, and soles were unaffected. She had known conditions of hypertension and diabetes, but her adherence to medications was poor. She had no history of allergies to food or drugs. Furthermore, her two pregnancies were uncomplicated.
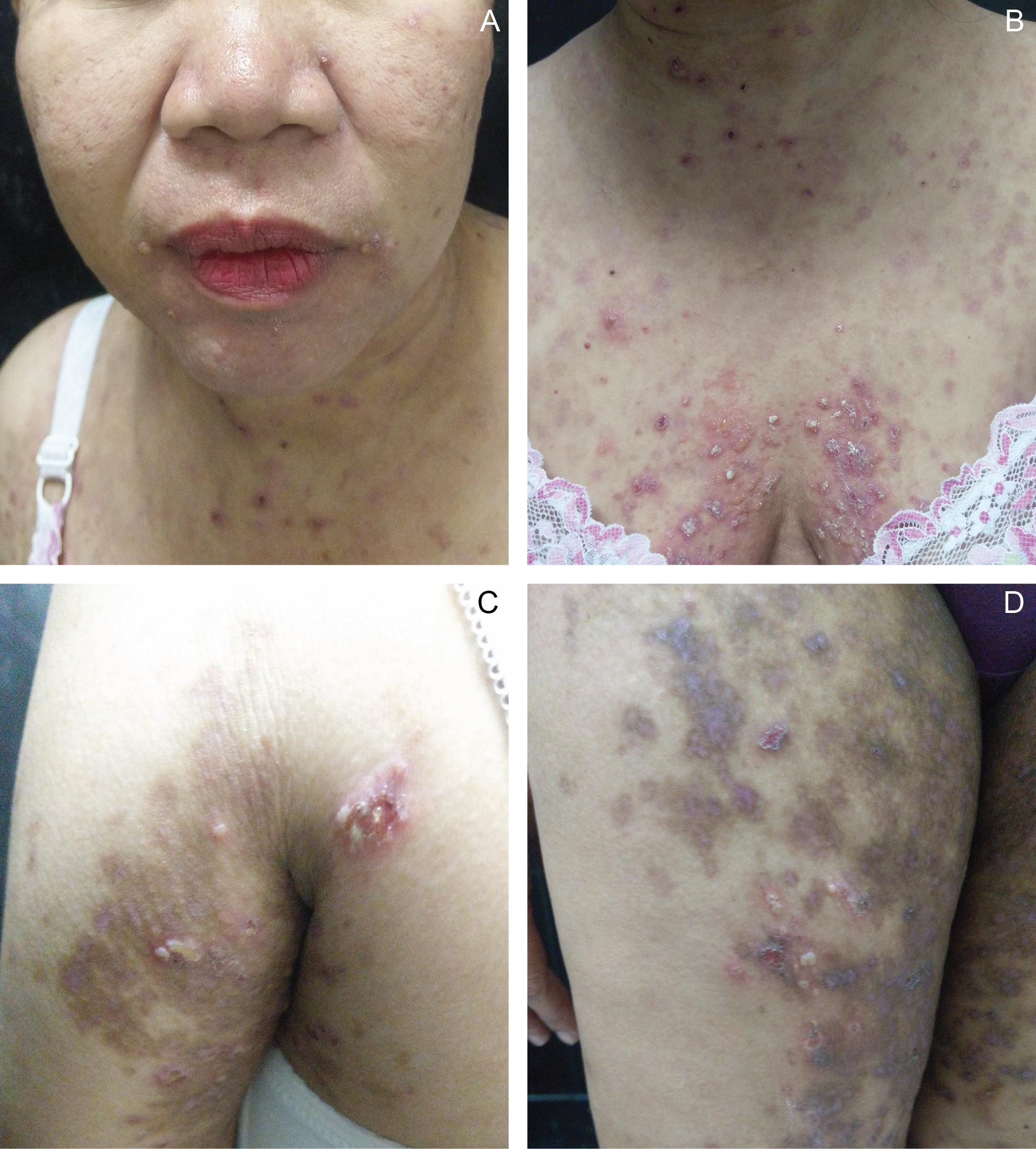
On physical examination (PE), there were multiple, varisized tense vesicles and erythematous urticarial plaques on the face, chest, and upper and lower extremities. The rest of the physical examination findings were unremarkable (Figure 1).
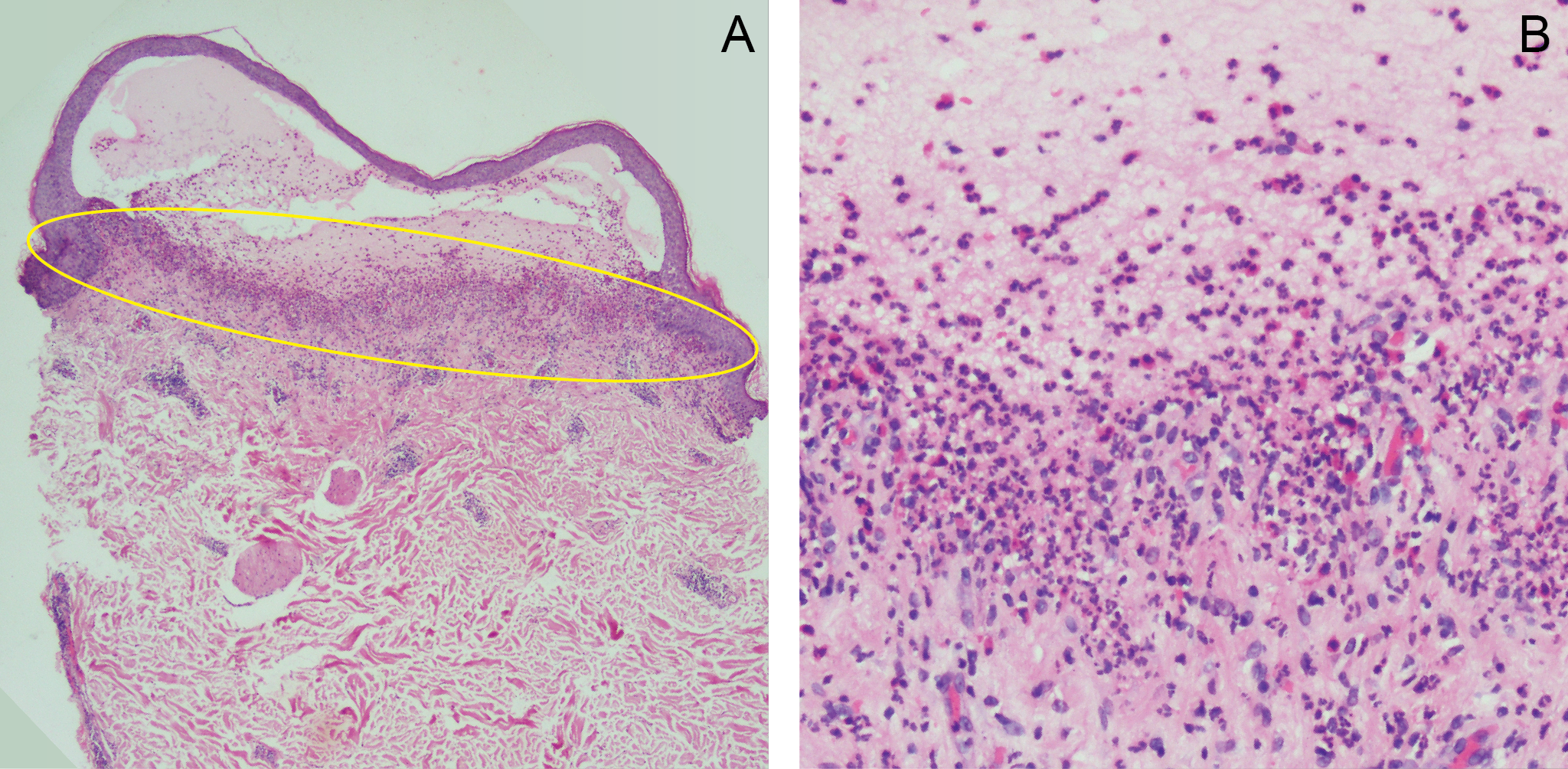
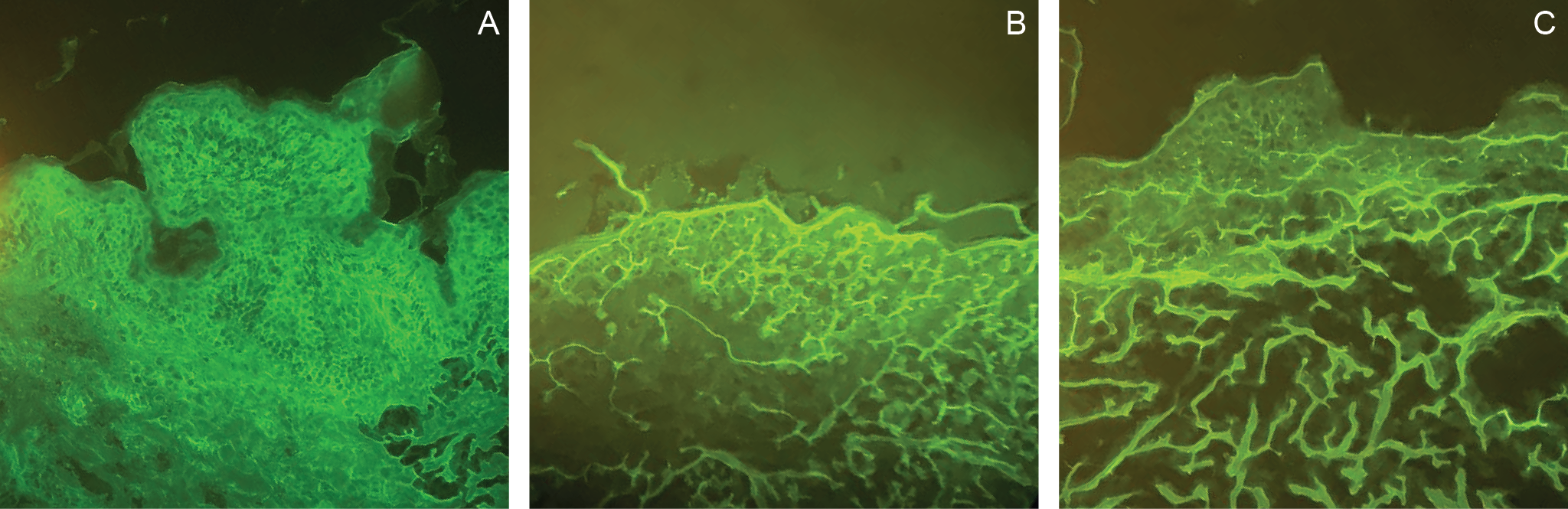
Based on the history and physical examination, our initial diagnosis was PG. We conducted a skin punch biopsy, taking specimens from a solitary vesicle and perilesional skin for hematoxylin and eosin staining and for direct immunofluorescence (DIF), respectively. The histopathology revealed an intact subepidermal vesicle with numerous eosinophils and neutrophils, particularly at the dermoepidermal junction (Figure 2), suggesting PG. However, DIF revealed intercellular IgA and faint linear IgM deposition, but no linear deposition of C3 and IgG, a hallmark finding for PG. (Figure 3) Furthermore, C4d immunohistochemistry of the formalin-fixed paraffin-embedded tissue was negative. This test is crucial to differentiate PEP from PG, as PG typically shows high positivity for C4d.9 Considering all these findings, we concluded that the patient’s condition was more consistent with PEP rather than PG.
During the patient’s initial consultation at our clinic, we prescribed clobetasol propionate ointment to be applied twice daily for two weeks. We also prescribed loratadine 10 mg to be taken in the morning and oral diphenhydramine 25 mg at bedtime. Our management plan also included a two-week course of prednisone. However, due to elevated blood glucose levels, this part of the treatment was not implemented. As new lesions appeared, the use of clobetasol propionate was extended for several more weeks. Regular follow-ups were conducted via teledermatology.
The unusual presentation of PEP can present a significant challenge in terms of patient and fetal management and prognosis. Our patient, who is multigravid, was in her first trimester of pregnancy when she began to exhibit cutaneous symptoms. She had lesions on her face, and her symptoms persisted even after childbirth. This is a stark departure from the typical presentation of PEP. Therefore, a thorough history and PE, supplemented by histology, immunofluorescence, and immunohistochemistry, are essential for distinguishing it from other gestational dermatoses, especially from PG, which can have implications for fetal outcomes.
 |
|
Figure 1 Multiple tense vesicles and erythematous urticarial plaques on the face (A), chest (B), and upper (C) and lower extremities (D) noted at 26 weeks postpartum. |
|
|
Figure 2 Histopathology of the skin lesion showing an intact subepidermal blister with numerous inflammatory infiltrates in the dermoepidermal junction, upper dermis, and superficial perivascular area (A: yellow ring). Magnified image of eosinophilic and neutrophilic infiltrates in the dermoepidermal junction (hematoxylin-eosin stain, A: scanning magnification and B: x40). |
|
|
Figure 3 Direct immunofluorescence of perilesional skin showing intercellular IgA deposition (A) and a negative IgG (B) and C3 (C) deposition in the basement membrane zone (A: scanning magnification, B: x10, C: x10). |
Contributors
AIC and MPB contributed to the diagnostic and therapeutic care of the patient in this report. All of them acquired relevant patient data, and searched for and reviewed relevant medical literature used in this report. AIC wrote the original draft, performed the subsequent revisions. All approved the final version, and agreed to be accountable for all aspects of this report.
Acknowledgments
We would like to thank Dr Jen-Christina Lourdes Segovia of the Department of Dermatology in Southern Philippines Medical Center (DD-SPMC) for her help in the management of the patient, and Dr Nadra Magtulis, also from the DD-SPMC, for her assistance in creating this case report.
Patient consent
Obtained
Article source
Submitted
Peer review
External
Competing interests
None declared
Access and license
This is an Open Access article licensed under the Creative Commons Attribution-NonCommercial 4.0 International License, which allows others to share and adapt the work, provided that derivative works bear appropriate citation to this original work and are not used for commercial purposes. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc/4.0/
References
1. Brandão P, Portela-Carvalho AS, Melo A, Leite I. Post-partum Polymorphic Eruption of Pregnancy. Obstet Gynecol Cases Rev. 2018; 5:139.
2. Pritzier EC, Mikkelsen CS. Polymorphic eruption of pregnancy developing postpartum: 2 case reports. Dermatol Reports. 2012 Jun 6;4(1):e7.
3. Pierson JC. Polymorphic Eruption of Pregnancy. 2020 Feb 21 [cited 2023 Oct 13]. In: Medscape. New York: Medscape. c1994-2023. Available from: https://emedicine.medscape.com/article/1123725-overview?form=fpf.
4. Oakley A. Polymorphic eruption of pregnancy. 2017 Sep [cited 2023 Oct 13]. In: DermNet. New Zealand: New Zealand. c2023. Available from: https://dermnetnz.org/topics/polymorphic-eruption-of-pregnancy.
5. Pomeranz MK. Dermatoses of pregnancy. 2023 Aug 23 [cited 2023 Oct 13]. In: UpToDate. Netherlands: Wolter Kulwer NV. c2023. Available from: https://www.uptodate.com/contents/dermatoses-of-pregnancy.
6. Mehedintu C, Isopescu F, Ionescu OM, Petca A, Bratila E, Cirstoiu MM, et al. Diagnostic Pitfall in Atypical Febrile Presentation in a Patient with a Pregnancy-Specific Dermatosis-Case Report and Literature Review. Medicina (Kaunas). 2022 Jun 25;58(7):847.
7. Calinescu A, Popescu R, Popescu CM, Hodorogea A, Brinzea A, Zeiler L, et al. Polymorphic Eruption of Pregnancy with Postpartum Onset: A Case Report. EMJ Dermatol. 2018;6(1):99-100.
8. Studdiford JS, George N, Trayes K. Pruritic Rash in Pregnancy. Am Fam Physician. 2017 Apr 1;95(7):453-454.
9. Kwon EJ, Ntiamoah P, Shulman KJ. The utility of C4d immunohistochemistry on formalin-fixed paraffin-embedded tissue in the distinction of polymorphic eruption of pregnancy from pemphigoid gestationis. Am J Dermatopathol. 2013 Dec;35(8):787-91.
Copyright © 2023 AI Contreras, et al.
Warning: mysqli_select_db() expects exactly 2 parameters, 1 given in /home/qrjicuku/public_html/V9N2Galley/Contreras/Contreras.php on line 385
Published
October 16, 2023
Issue
Volume 9 Issue 2 (2023)
Section
Case in images

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Authors who publish with this journal agree to the following terms:
- Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution-NonCommercial 4.0 International License that allows others to share the work for non-commercial purposes with an acknowledgement of the work's authorship and initial publication in this journal.
- Authors are able to enter into separate, additional, non-commercial contractual arrangements for the non-exclusive distribution of the journal's published version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgement of its initial publication in this journal.
- Authors grant the journal permission to rewrite, edit, modify, store and/or publish the submission in any medium or format a version or abstract forming part thereof, all associated supplemental materials, and subsequent errata, if necessary, in a publicly available publication or database.
- Authors warrant that the submission is original with the authors and does not infringe or transfer any copyright or violate any other right of any third parties.