Implementation of trauma protocols in Southern Philippines Medical Center in 2024
SPMC J Health Care Serv. 2024;10(2):2 ARK: https://n2t.net/ark:/76951/jhcs56hd6r
1Department of Emergency Medicine, Southern Philippines Medical Center, J.P. Laurel Avenue, Bajada, Davao City
2Research Utilization and Publication Unit, Southern Philippines Medical Center, JP Laurel Ave, Davao City, Philippines
Correspondence Kenny Gene R Salvador, kensalvador24@gmail.com
Received 2 April 2024
Accepted 29 November 2024
Cite as Salvador KGR, Valdez BEP, Ladrero CXDL. Implementation of trauma protocols in Southern Philippines Medical Center in 2024. SPMC J Health Care Serv. 2024;10(2):2. https://n2t.net/ark:/76951/jhcs56hd6r
Clinical protocols, pathways, and algorithms are not just guidelines, but life-saving tools in the management of trauma.1 By standardizing care, reducing variability, and improving patient outcomes, they provide health care professionals with evidence-based guidelines to ensure timely and effective treatment.2 3 In the fast-paced and high-stakes environment of trauma care, these structured approaches have been shown to decrease mortality rates and complications, leading to better overall patient recovery.
The World Health Organization (WHO) has been a global leader in the development of trauma care protocols, aiming to enhance the quality of emergency services on an international scale. Their initiatives, such as the WHO Trauma Care Checklist4 and the Guidelines for Essential Trauma Care,5 have provided frameworks for health care systems worldwide to better prepare for and respond to trauma incidents.6 The implementation of these protocols in various countries has led to significant improvements in patient survival rates and reductions in trauma-related disabilities. Notably, in low-resource settings, adherence to WHO guidelines has resulted in more efficient use of available resources and improved clinical outcomes.7
The Southern Philippines Medical Center (SPMC) in Davao City is the leading hospital in Mindanao, renowned for its trauma care and its designation as a Level I trauma center, catering to approximately 1,300 patients monthly. Equipped with cutting-edge facilities and a specialized team, SPMC manages severe trauma cases and offers comprehensive care from initial treatment to surgical intensive care. The hospital also plays a crucial role in training and research, collaborating with various organizations to advance trauma care and maintain its leadership in emergency medical services in the region.
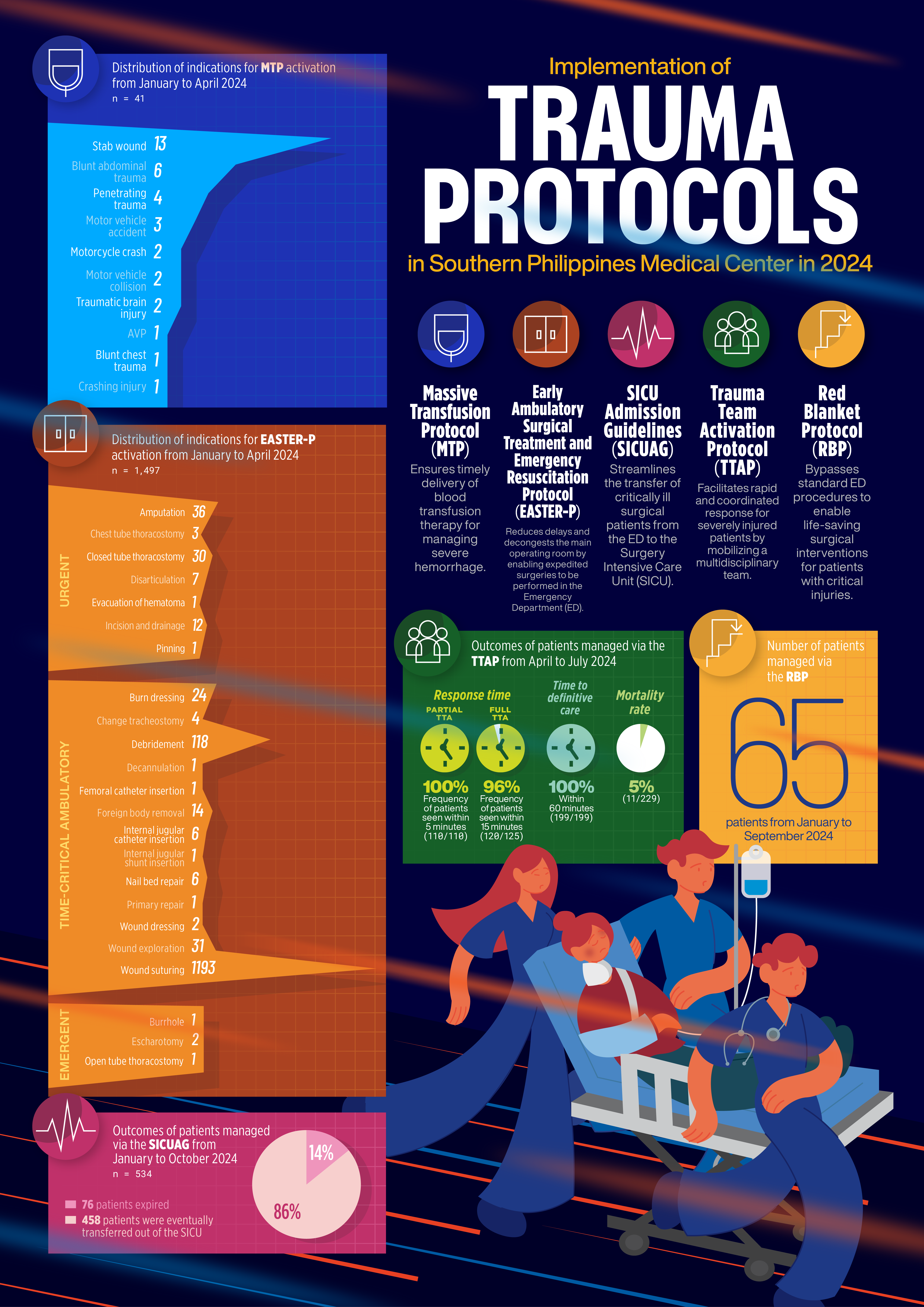
The SPMC Institute of Emergency, Acute, Trauma, and Critical Care (IEATCC) provides rapid, coordinated, and life-saving interventions to enhance patient safety and well-being. It leads efforts to reduce trauma-related mortality and morbidity through comprehensive, evidence-based care from pre-hospital to intensive care. The institutionalization of emergency trauma and critical care in 2022, as recognized by the Society for the Surgery of Trauma under the Philippine College of Surgeons, has led to the establishment of several key initiatives. These include Trauma Team Activation Protocol (TTAP), Massive Transfusion Protocol (MTP), Red Blanket Protocol (RBP), and the Surgical Intensive Care Unit Admission Guidelines (SICUAG). Additionally, the Early Ambulatory Surgical Treatment and Emergency Resuscitation (EASTER) protocol, developed in 2016, has been integrated into these efforts.
These initiatives are designed as a comprehensive bundle rather than standalone systems, significantly enhancing the efficiency of trauma management. Integrating these protocols and guidelines as a cohesive package ensures a more streamlined approach. Emphasizing efficiency monitoring and fostering intercommunication among these functions is crucial for their success.
Trauma Team Activation Protocol
The Trauma Team Activation (TTA) strategy has been adopted and formally implemented in January 2024. It mobilizes a multidisciplinary team that ensures a rapid, coordinated response for severely injured patients, improving outcomes through faster time-to-treatment, supported by Davao City's Central 911 EMS partnership and prehospital notifications. Partial trauma team activation involves emergency medicine physicians, trauma surgeons and trauma resuscitation nurses, while full trauma team activation included a multidisciplinary team, consisting of doctors and staff from Emergency Medicine, Orthopedics, Trauma Surgery, Neurosurgery, Interventional Radiology, Internal Medicine, Pediatrics, Anesthesia, and more. The success of the TTAP underscores the critical role of interdisciplinary teams in trauma care. By combining specialized expertise, they ensure holistic management, streamline decisions, minimize delays, and enhance patient outcomes. To ensure effective monitoring of this protocol, each TTA is logged in a real-time online database and registry for Emergency Medicine.
Despite challenges like limited resources, an overcrowded emergency department, and inconsistent activation, all patients requiring partial trauma team activation (110/110; 100%) received it within 5 minutes, while nearly all needing full activation (120/125; 96%) received it within 15 minutes from April 2024 to July 2024. During the same period, for all 199 patients with available data on arrival time and time of definitive care, care was provided within 60 minutes of arriving at the ED (100%). The emergency department trauma mortality rate for severe trauma cases was 4.80%.
Massive Transfusion Protocol
The MTP was officially implemented in January 2024. Our partners in the Department of Laboratory and Pathological Sciences, together with the SPMC Blood Bank, supported the IEATCC in implementing the MTP. This protocol is crucial for managing severe hemorrhage in trauma patients, ensuring the timely and effective delivery of balanced transfusion therapy. It aligns with the Universal Health Care’s emphasis on comprehensive care and an integral role in reducing preventable deaths within a well-coordinated trauma system.
The MTP was activated for 36 trauma patients from January 2024 to April 2024, with an average time to the first transfusion of 17.24 ± 6.79 minutes (n=17). On average, 104 units of blood were requested per month through the protocol, but only 63 units were actually used. Per patient, an average of 10 units was requested, while only 6 units were used.
Early Ambulatory Surgical Treatment and Emergency Resuscitation protocol
The Early Ambulatory Surgical Treatment and Emergency Resuscitation (EASTER) protocol, introduced in 2018, expedites surgeries at the ED, reducing delays, decongesting the main operating room, and minimizing trauma-related morbidities. The EASTER unit comprises two sterile rooms, capable of accommodating 3-4 surgical procedures simultaneously, depending on the case. It is staffed by nurses trained in surgical procedures, supported by a nurse attendant. The unit primarily handles trauma and orthopedic cases, performing procedures such as wound repair, debridement, and closed fracture reductions. It is also equipped for cranial burr-holing, central-line placement, and chest tube insertions. Peripheral nerve blocks and sedation are routinely used for pain management.
From January to April 2024, 1,524 ED patients, with a mean age of 31 years, activated the EASTER protocol. Most of the procedures (1,402/1,497; 93.72%) fell under the category of ‘time-critical ambulatory procedures,’ such as wound suturing, wound exploration, debridement, foreign body removal. Urgent procedures accounted for 6.02% (90/1,497), while only 0.27% (4/1,497) were emergent procedures. The average time it took from requesting the procedure to the starting of the procedure was 135 ± 399 minutes (n=724), and the average procedure duration was 24 ± 19 minutes (n=364). Since its implementation, the EASTER protocol has improved surgical response times and patient outcomes, but resource and infrastructure constraints, staffing shortages, and inconsistent adherence limit its broader effectiveness.
Surgical Intensive Care Unit Admission Guidelines
Admission to the Surgical Intensive Care Unit (SICU) is indicated for critically-ill surgical patients, including preoperative, postoperative cases, and non-operative cases. The SICUAG, introduced in early 2024, aims to provide evidence-based, optimal care to critically injured patients. Transitioning to a semi-open SICU model introduced a dedicated trauma and critical care physician, ensuring 24/7 presence and streamlined patient management. This shift improved subspecialty coordination, prioritized admissions based on clinical need, and enabled integrated, timely care through a multidisciplinary team approach.
From January 2024 to October 2024, the protocol was applied to 534 patients, averaging 53 admissions monthly. Of these, 76 (14.23%) patients expired during their ICU stay, while the remaining 458 (85.77%) were eventually transferred out of the SICU. Preliminary observations indicate increased direct admissions from the ED and reduced morbidity and mortality, although comprehensive data analysis is ongoing. A key challenge in implementing the SICU admission guidelines is adapting from a traditional open ICU model to a semi-open ICU model, which poses a learning curve for other departments, particularly in centralizing patient care within the SICU. However, prioritizing evidence-based practices and best-practice implementation is essential to achieving a more seamless and coordinated approach to managing critically ill patients.
Red Blanket Protocol
The RBP, introduced in 2022, aims to expedite life-saving surgical interventions for critically injured patients by bypassing standard ED procedures. This direct-to-operating-room strategy significantly reduces delays for patients with life-threatening conditions, such as those with major hemorrhages from blunt or penetrating injuries, improving survival rates and minimizing complications. From January to September 2024, the protocol was activated for 65 patients, averaging 7 cases per month, mean ED to OR time of 75 minutes and mortality rate of 9.2%, often attributed to severity of injury.
Since the implementation of the RBP, there has been a notable improvement in mortality and morbidity trends, as well as a reduction in the turnaround time for transporting trauma patients to the operating room for definitive care. Successful implementation relies on seamless coordination among trauma teams, surgical staff, and operating room preparedness. Challenges include resource limitations and ensuring strict adherence to activation criteria. Addressing these barriers can enhance the protocol's effectiveness.
The implementation of trauma protocols at SPMC offers several gains and opportunities for improvement. We aspire for our efforts to be recognized for exemplifying practices aligned with the principles espoused by the WHO for effective trauma care systems. These efforts improve patient outcomes and position SPMC as a model for adopting evidence-based practices in local and global health care. Documenting and publishing our system provides a useful resource for other hospitals with similar patient volumes, enabling adaptation to their specific contexts. It also opens avenues for international, national and local practitioners to rotate through SPMC and learn from its approach, fostering training, education, and professional linkages. Expanding EASTER services to include additional procedures enhances patient care offerings. Nurses’ involvement in the trauma system fosters workforce development and underscores the collaboration of physicians, nurses, paramedics, and support staff, ensuring effective care. Lastly, follow-up review studies and related research are planned after this publication to further expand insights and ensure continuous improvement.
In the future, the SPMC IEATCC plans to integrate these trauma protocols bundle with rehabilitation systems to ensure seamless patient reintegration to the community. Specific strategies to overcome identified challenges include establishing partnerships with the community, rehabilitation centers, leveraging telemedicine for follow-up care, and training health care providers in holistic, post-discharge management. Additionally, the ‘bundles of trauma care’ will be developed into a structured learning curriculum, while data from our experience will support efforts in standardizing trauma prevention initiatives.
Future research directions will focus on evaluating long-term impact of these protocols on patient outcomes, identifying gaps in care, and exploring innovative approaches to trauma management. Moreover, regular training workshops will be implemented to refine the skills of health care professionals, fostering a culture of continuous learning and quality improvement.
The SPMC IEATCC strives to redefine trauma care standards, aligning with the commitment of SPMC to high-quality, equitable, and comprehensive patient care. Through advanced trauma protocols and continuous staff development, SPMC seeks to improve patient outcomes, reduce mortality rates, and minimize trauma-related complications, solidifying its role as a premier health care provider for Mindanao.
Contributors
KGRS and BEPV conceptualized the article. KGRS, and BEPV wrote the original draft, while CXDL rendered the original draft of the infographic. All authors performed the subsequent revisions, approved the final version, and agreed to be accountable for all aspects of this article and its corresponding infographic.
Article source
Commissioned
Peer review
External
Competing interests
None declared
Access and license
This is an Open Access article licensed under the Creative Commons Attribution-NonCommercial 4.0 International License, which allows others to share and adapt the work, provided that derivative works bear appropriate citation to this original work and are not used for commercial purposes. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc/4.0/
References
1 Büscher A, Kugler J. The effectiveness of clinical pathways in inpatient settings - an umbrella review. J Public Health (Berl.). 2024.
2 Jarman H, Crouch R, Halter M, Peck G, Cole E. Provision of acute care pathways for older major trauma patients in the UK. BMC Geriatr. 2022 Nov 29;22(1):915.
3 Allum L, Apps C, Hart N, Pattison N, Connolly B, Rose L. Standardising care in the ICU: a protocol for a scoping review of tools used to improve care delivery. Syst Rev. 2020 Jul 19;9(1):164.
4 World Health Organization. Trauma care checklist. 2016 [cited 2024 Dec 11]. In: World Health Organization [Internet]. Geneva: World Health Organization. Available from: https://www.who.int/publications/i/item/trauma-care-checklist
5 Mock C, Lormand JD, Goosen J, Joshipura M, Peden M. Guidelines for essential trauma care. World Health Organization. 2004. Available from: https://iris.who.int/bitstream/handle/10665/42565/9241546409_eng.pdf?sequence=1&isAllowed=y
6 Bidhendi S, Ahmadi A, Fouladinejad M, Bazargan-Hejazi S. Evaluating implementation of WHO Trauma Care Checklist vs. modified WHO checklist in improving trauma patient clinical outcomes and satisfaction. J Inj Violence Res. 2021 Jan;13(1):5-12.
7 Whitaker J, O'Donohoe N, Denning M, Poenaru D, Guadagno E, Leather AJM, et al. Assessing trauma care systems in low-income and middle-income countries: a systematic review and evidence synthesis mapping the Three Delays framework to injury health system assessments. BMJ Glob Health. 2021 May;6(5):e004324.
Copyright © 2024 KGR Salvador, et al.

Published
December 11, 2024
Issue
Volume 10 Issue 2 (2024)
Section
Infographic

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Authors who publish with this journal agree to the following terms:
- Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution-NonCommercial 4.0 International License that allows others to share the work for non-commercial purposes with an acknowledgement of the work's authorship and initial publication in this journal.
- Authors are able to enter into separate, additional, non-commercial contractual arrangements for the non-exclusive distribution of the journal's published version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgement of its initial publication in this journal.
- Authors grant the journal permission to rewrite, edit, modify, store and/or publish the submission in any medium or format a version or abstract forming part thereof, all associated supplemental materials, and subsequent errata, if necessary, in a publicly available publication or database.
- Authors warrant that the submission is original with the authors and does not infringe or transfer any copyright or violate any other right of any third parties.