Health care approach to burn mass casualty incidents: policy notes
SPMC J Health Care Serv. 2024;10(1):5 ARK: https://n2t.net/ark:/76951/jhcs2g3q4f
1Department of Emergency Medicine, Southern Philippines Medical Center, JP Laurel Avenue, Bajada, Davao City
2Research Utilization and Publication Unit, Southern Philippines Medical Center, JP Laurel Ave, Davao City, Philippines
Correspondence Benedict Edward P Valdez, rbenz628@gmail.com
Received 15 March 2024
Accepted 5 June 2024
Cite as Valdez BEP, Paderanga MAR, David JDM, Perandos-Astudillo CM, Roño RC. Health care approach to burn mass casualty incidents: policy notes. SPMC J Health Care Serv. 2024;10(1):5. https://n2t.net/ark:/76951/jhcs2g3q4f
Introduction
A burn mass casualty incident (BMCI), an incident that involves at least three burn victims with severe injuries,1 presents several unique challenges. In a mass casualty event, between 25 and 30 percent of those injured can sustain moderate-to-severe burn injuries.2 Management of burn patients necessitates a significant amount of health resources and logistical support, along with prompt and high-quality care to optimize the functional and cosmetic outcomes of severely injured patients. While some developed countries have sound disaster management plans, many countries where most BMCIs occur lack such well-established plans.3
The effective management of BMCIs is crucial for positive patient outcomes. Given resource scarcity, especially in geographically isolated and disadvantaged areas, comprehensive mitigation and preparedness strategies are essential. These strategies must address worst-case scenarios that may challenge the existing internal protocols, especially at the local level.4 The surge in health care facility capacity during BMCIs can quickly overwhelm local and regional resources, from prehospital care to specialized burn centers. In the Philippines, disaster response levels and adequacy may vary widely among different regions and local government units (LGU). While the Department of Health has issued guidelines for health emergency and disaster response management,5 there are currently no policies or guides on specifically addressing preincident planning for BMCIs.
The aim of this article is to recommend policies that will potentially improve the current health care approach to BMCIs.
Main evidence
The Health Care Focus article by Paderanga, et al in March 20241 provides a thorough description of the management of BMCIs based on their experience responding to the C-130 military aircraft crash in Patikul, Sulu on July 4, 2021. In the Patikul incident, more than half of the 104 personnel on board and on the ground were killed, while others sustained multiple injuries. The injured casualties had a combination of cutaneous burns, inhalational injury, and other traumatic injuries, necessitating a multidisciplinary team of highly trained medical personnel and emergency authorities to manage on-scene operations. This event posed a significant challenge to the LGU where it occurred, prompting an immediate mobilization of resources and personnel. The Southern Philippines Medical Center (SPMC), the sole facility in Mindanao capable of handling massive and severe burn cases, dispatched a team of six doctors and one nurse to Zamboanga City 24 hours after the crash.
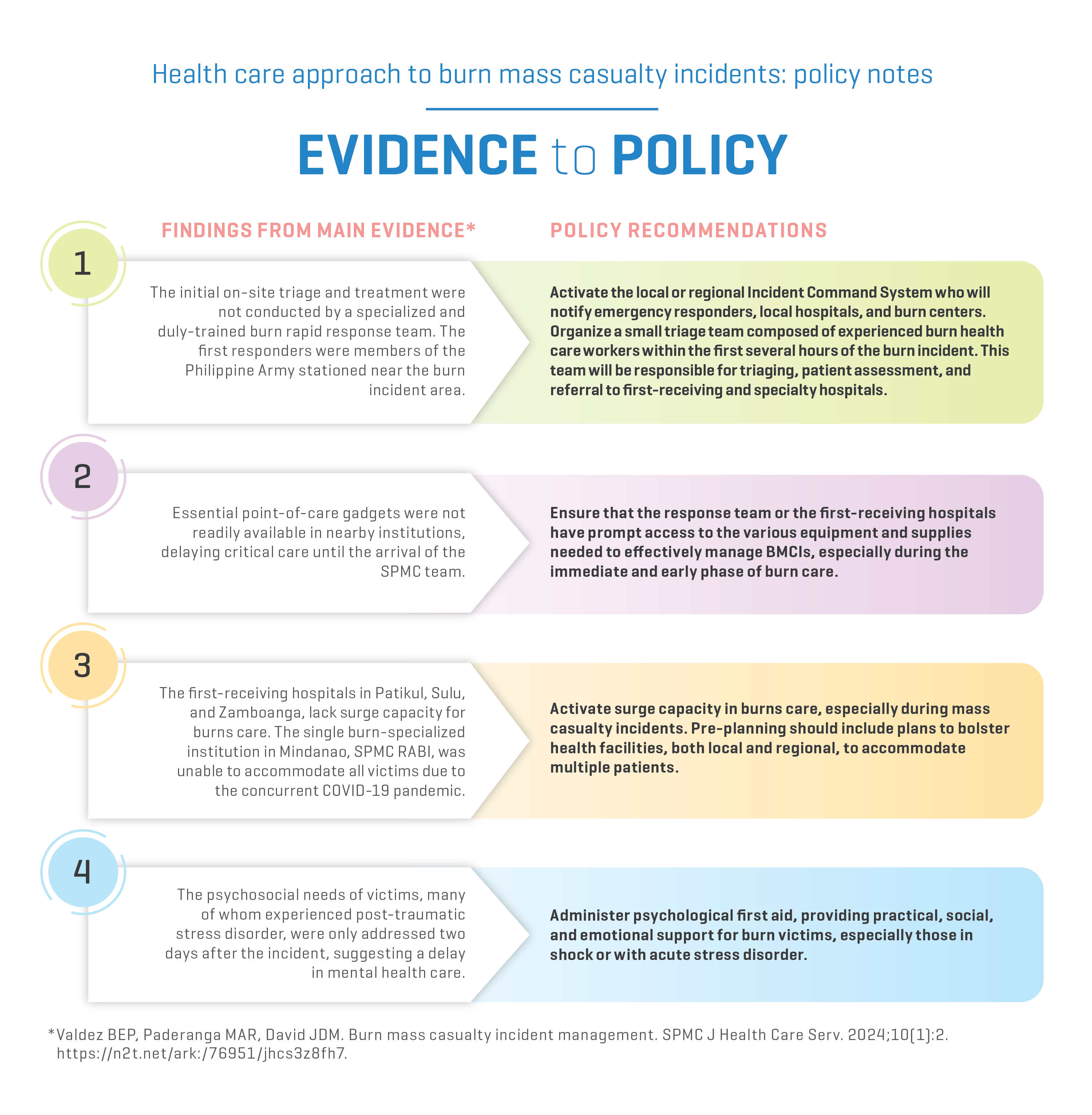
In the Patikul incident, several gaps in the health care system were identified. During the immediate aftermath of the disaster, the Joint Task Force Sulu of the Philippine military served as the first responders, conducting a search and rescue operation and performing on-site triage and treatment for the survivors. In the early phase of the response, burn care equipment, medicines, and medical supplies were not readily available in nearby institutions (usually first-receiving hospitals), causing delays, especially in the management of patients with severe burn injuries. At the SPMC Rizal Aportadera Burn Institute (RABI), only five survivors with severe burn injuries were accommodated, especially since the disaster occurred during the COVID-19 pandemic when SPMC became the main receiving center for COVID-19 cases in the region. Mental health and psychosocial support, as well as social services, arrived only a few days after the incident.
In the evidence-to-policy diagram below, we summarize key findings from the Health Care Focus article and provide policy recommendations.
Evidence-to-policy diagram
|
Related evidence
Disaster management in BMCIs requires coordination across health disciplines to prevent disasters, respond immediately, and rehabilitate victims. Effective disaster plans can mitigate property loss, social disruption, and suffering. 6 Comprehensive and properly designed BMCI plans, adequate resources, command control systems, and stakeholder participation are vital for effective response.4 7 The World Health Organization Emergency Medical Teams Technical Working Group on Burns outlines key themes for managing BMCIs, emphasizing patient distribution, fluid management, first aid, surgical interventions, rehabilitation, burn teams, training, infrastructure, and mass casualty planning.3
Initial care at disaster sites is often provided by survivors or passersby, and later supported by trained health care workers who administer first aid, perform patient triage, and allocate resources. An organized disaster response system, which includes medical, public safety, law enforcement, and transport agencies, is essential for effective management.6 Burn teams should be trained and self-sufficient. Effective triage by a specialized burn rapid response team is crucial during the initial phase.3
In 2012, the Incident Command System (ICS) was established as an on-scene disaster response and management mechanism under the Philippine Disaster Risk Reduction and Management System.8 Following a mass casualty incident, the local disaster plan must be put into action. A local or regional ICS directs command and control, triage, communication, and patient transfer,9 while the local Disaster Risk Reduction and Management Council Operations Center coordinates interagency relations, leveraging each agency’s resources for a cohesive and collaborative response.8 10
Burn care is resource-intensive. It requires adequate burn care equipment, medicines, and supplies for an organized response, and the responding burn team should have access to these resources. During BMCIs, even a few severe burn cases can significantly strain hospital resources, necessitating increased allocation. The need for IV fluids to prevent complications like hypovolemic shock and acute kidney injury is critical,11 and first-aid measures such as cooling and dressing play a vital role in improving outcomes.12
During mass casualty incidents, activating surge capacity in burn care is crucial. Pre-planning should focus on bolstering local and regional health facilities to accommodate multiple burn patients.3 5 Current protocols may fall short in such settings, where the complexity of injuries overwhelms health systems. Surge resource planning at local, regional, and national levels is essential. BMCIs pose challenges due to specialized burn care requirements, often concentrated in burn centers. Personnel at other hospitals must provide extended burn care despite limited experience. Non-burn surgeons can perform escharotomy and fasciotomy,13 while excision and grafting require skilled burn surgeons. Early rehabilitation minimizes contractures and maximizes functionality, involving multidisciplinary care and patient-family collaboration.14 15
Rehabilitation should encompass physical, psychological, and social aspects of care3 16 Addressing mental health needs within the first 48 hours is essential.5 17 Providing psychological first aid, including practical, social, and emotional support for burn victims, especially those who are in shock or with acute stress disorder, is crucial.18
Effective BMCI management requires thorough planning, resource allocation, and coordinated efforts among health care workers and agencies, ensuring each patient receives appropriate care based on their specific injuries.
Contributors
BEPV, MARP, JDMD, CMPA and RCR contributed to the conceptualization of this article. All authors wrote the original draft, performed the subsequent revisions, approved the final version, and agreed to be accountable for all aspects of this report.
Article source
Commissioned
Peer review
Internal
Competing interests
None declared
Access and license
This is an Open Access article licensed under the Creative Commons Attribution-NonCommercial 4.0 International License, which allows others to share and adapt the work, provided that derivative works bear appropriate citation to this original work and are not used for commercial purposes. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc/4.0/.
References
1 Gauglitz GG. Overview of the management of the severely burned patient. 2023 Nov 15 [cited 2024 Jun 18]. In: UpToDate [Internet]. Illinois: UpToDate, Inc. c2024. Available from: https://www.uptodate.com/contents/overview-of-the-management-of-the-severely-burned-patient/print.
2 Hughes A, Almeland SK, Leclerc T, Ogura T, Hayashi M, Mills JA, et al. Recommendations for burns care in mass casualty incidents: WHO Emergency Medical Teams Technical Working Group on Burns (WHO TWGB) 2017-2020. Burns. 2021 Mar;47(2):349-370.
3 Kearns RD, Marcozzi DE, Barry N, Rubinson L, Hultman CS, Rich PB. Disaster Preparedness and Response for the Burn Mass Casualty Incident in the Twenty-first Century. Clin Plast Surg. 2017 Jul;44(3):441-449.
4 Department of Health Philippines. MANUAL OF OPERATIONS on Health Emergency and Disaster Response Management. 2015. Available from: https://hospitalsafetypromotionanddisasterpreparedness.wordpress.com/wp-content/uploads/2015/11/complete-manual-20150129.pdf
5 Valdez BEP, Paderanga MAR, David JDM. Burn mass casualty incident management. SPMC J Health Care Serv. 2024;10(1):2. https://n2t.net/ark:/76951/jhcs3z8fh7
6 Ahuja RB, Bhattacharya S. Burns in the developing world and burn disasters. BMJ. 2004 Aug 21;329(7463):447-9.
7 Kearns RD, Conlon KM, Valenta AL, Lord GC, Cairns CB, Holmes JH, et al. Disaster planning: The basics of creating a burn mass casualty disaster plan for a burn center. Journal of Burn Care & Research. 2014 Jan 1;35(1):e1-e13.
8 National Disaster Risk Reduction and Management Council. Implementing guidelines on the use of Incident Command System (ICS) as on-scene disaster response and management mechanism under Philippine Disaster Risk Reduction and Management System (PDRRMS), Memorandum Circular No. 04 Series 2012, 2012 Mar 28.
9 Crossett JR, Peterson WC, King BT. Burn mass casualty disaster. Medical Research Archives. 2018;6(8).
10 Restrata. Incident command system for more effective crisis management. Available from: https://www.restrata.com/blog/incident-command-system-for-more-effective-crisis-management/
11 Lyall A, Bhadauria AS. Fluid management in major burns. 2024 [cited 2024 Jun 18]. In: Malbrain ML, Wong A, Nasa P, Ghosh S, editors. Rational use of intravenous fluids in critically ill patients. New York: Springer. Available from: https://link.springer.com/chapter/10.1007/978-3-031-42205-8_19.
12 Hudspith J, Rayatt S. First aid and treatment of minor burns. BMJ. 2004 Jun 19;328(7454):1487-9.
13 Streitz MJ. How to do burn escharotomy. 2023 Apr [cited 2024 Jun 18]. In: MSD Manual Professional Version [Internet]. New Jerser: Merck & Co., Inc. c2024. Available from: https://www.msdmanuals.com/professional/injuries-poisoning/how-to-do-skin,-soft-tissue,-and-minor-surgical-procedures/how-to-do-burn-escharotomy.
14 Hayashi K, Sasabuchi Y, Matsui H, Nakajima M, Otawara M, Ohbe H, et al. Does early excision or skin grafting of severe burns improve prognosis? A retrospective cohort study. Burns. 2023 May;49(3):554-561.
15 Goswami P, Sahu S, Singodia P, Kumar M, Tudu T, Kumar A, et al. Early Excision and Grafting in Burns: An Experience in a Tertiary Care Industrial Hospital of Eastern India. Indian J Plast Surg. 2019 Sep;52(3):337-342.
16 Procter F. Rehabilitation of the burn patient. Indian J Plast Surg. 2010 Sep;43(Suppl):S101-13.
17 Fetter JC. Psychosocial Response to Mass Casualty Terrorism: Guidelines for Physicians. Prim Care Companion J Clin Psychiatry. 2005;7(2):49-52.
18 European Federation of Psychologists Associations. Lessons learned in psychosocial care after disasters. Council of Europe. 2010 Jul. Available from: https://www.coe.int/t/dg4/majorhazards/ressources/pub/Lessonslearned_Oct2010_EN.pdf.
Copyright © 2024 BEP Valdez, et al.

Published
June 18, 2024
Issue
Volume 10 Issue 1 (2024)
Section
Policy notes

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Authors who publish with this journal agree to the following terms:
- Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution-NonCommercial 4.0 International License that allows others to share the work for non-commercial purposes with an acknowledgement of the work's authorship and initial publication in this journal.
- Authors are able to enter into separate, additional, non-commercial contractual arrangements for the non-exclusive distribution of the journal's published version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgement of its initial publication in this journal.
- Authors grant the journal permission to rewrite, edit, modify, store and/or publish the submission in any medium or format a version or abstract forming part thereof, all associated supplemental materials, and subsequent errata, if necessary, in a publicly available publication or database.
- Authors warrant that the submission is original with the authors and does not infringe or transfer any copyright or violate any other right of any third parties.