Endogenous Klebsiella pneumoniae panophthalmitis with perinephric and psoas abscesses in a 42-year-old female: case in images
SPMC J Health Care Serv. 2020;6(1):8 ARK: https://n2t.net/ark:/76951/jhcs39brs9
1Department of Ophthalmology, Southern Philippines Medical Center, JP Laurel Ave, Davao City, Philippines
Correspondence Charmaine Grace P Malabanan-Cabebe, charmainegrace.0923@gmail.com
Received 2 March 2020
Accepted 29 June 2020
Cite as Malabanan-Cabebe CGP, Villano MAF. Endogenous Klebsiella pneumoniae panophthalmitis with perinephric and psoas abscesses in a 42-year-old female: case in images. SPMC J Health Care Serv. 2020;6(1):8. https://n2t.net/ark:/76951/jhcs39brs9
Endophthalmitis is the inflammation of the intraocular cavities, and panophthalmitis is its most severe form.1 2 3 In panophthalmitis, there is a marked inflammation of the surrounding orbital structures, manifested by severe eyelid edema, proptosis, chemosis and eye movement limitations.4 If left untreated, endophthalmitis could lead to irreversible vision loss and systemic complications.2 4 5
The etiology of endophthalmitis may either be exogenous, by direct inoculation, or endogenous, via hematogenous spread of infectious agents from a distant source.4 6 7 Occurring less commonly than its exogenous counterpart, endogenous endophthalmitis (EE) accounts for only 2 to 15% of all endophthalmitis cases.1 6 7 Gram-negative rods, such Klebsiella pneumoniae are responsible for most of the cases of EE in Asian countries.8 9 10 The most common symptom of endophthalmitis is decreased visual acuity and hypopyon, or pus in the anterior chamber.6 4 11 The diagnosis of endophthalmitis is established through characteristic B-scan ultrasonographic findings such as increased echogenicity of the vitreous, retinochoroidal layer thickening, and retinal detachments.12 13 Other diagnostic procedures that are commonly done are vitreous fluid biopsy, blood culture (which is positive in only a third of cases) and neuroimaging (to evaluate the presence of intraocular foreign body, or sources of intraorbital or intraocular infection).14 15 16 Treatment should be started upon suspicion of endophthalmitis. Treatment usually includes the administration of intravitreal and intravenous systemic antibiotics.14 7 Pars plana vitrectomy is used to treat moderate vitritis.14 It is usually done on patients in the early course of infection, when there is still low virulence of the infective organism.18 Endophthalmitis caused by a gram-negative organism tends to have poor visual acuity outcomes.2 In extreme cases of endophthalmitis, enucleation or evisceration may have to be performed as the last option to control the progress of infection.3
A 42-year-old female complaining of right-eye swelling was admitted under our service. Forty days prior to admission, the patient had fever and chills associated with left flank pain, cloudy urine and bilateral leg edema. About a week after the onset of symptoms, she was admitted for a complicated urinary tract infection (UTI) secondary to nephrolithiasis, given intravenous ceftriaxone, and eventually discharged after ten days, with resolution of symptoms, except for the persistence of minimal left flank pain.
The swelling in the patient’s right eye started five days prior to admission and was associated with eye pain. Four days prior to admission, the patient consulted a physician and was prescribed with unrecalled antibiotic eye drops. Two days prior to admission, when the eyedrops did not afford any relief of the symptoms, the patient consulted a second physician who prescribed acetazolamide 250 mg tablet, one tablet twice a day and levofloxacin 0.5% eye drops, one drop every four hours on the right eye. However, the condition of the patient's right eye did not improve the next day, despite the new medications. She went back to the second doctor, who then made a diagnosis of panophthalmitis and referred her to our institution for further management.
The patient has been diagnosed to have a poorly-controlled diabetes mellitus type 2 for a year now, and she has been poorly compliant with her insulin treatment. The patient denied any recent history of dysuria, hematuria, abdominal pain or changes in bowel movement.
On initial examination, we noted a hyperemic sclera and discharges on the patient’s right eye. Visual acuity test revealed that she had no light perception on the right eye but had 20/20 vision on the left eye. The examination also revealed a grossly edematous, erythematous, and proptotic right eye with severely restricted extraocular movements (Figure 1).
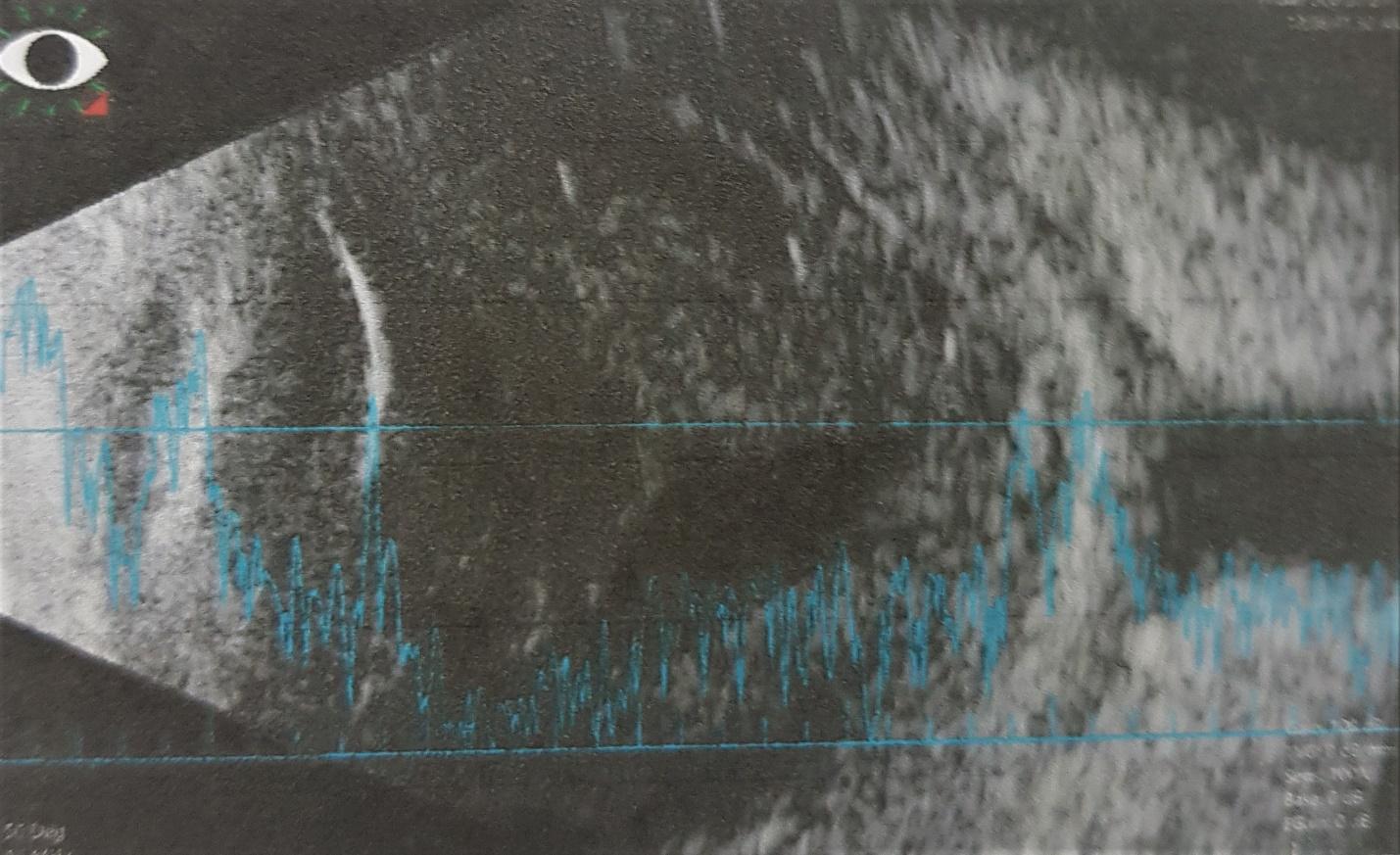
Slit lamp biomicroscopy showed severe diffuse conjunctival injection with perilimbal thickening, mucoid discharge, diffuse corneal edema, and profuse fibrin formation in the anterior chamber (Figure 2). There was no view of the posterior pole due to the fibrin formation and corneal edema. Intraocular pressure was elevated to 42 mmHg on applanation tonometry. Ophthalmic ultrasonography revealed homogeneous hyperechoic dots of low- to mid-reflectivity, with good after-movement. The choroid was thickened (Figure 3).
We admitted the patient with a working diagnosis of endophthalmitis. We then performed a vitreous tap, collected a sample of vitreous fluid for culture, and injected 0.1 ml vancomycin with 1 mg/0.1 mL preparation and 0.1 ml ceftazidime with 2.25 mg/0.1 mL preparation. We also collected blood and urine samples for culture before we started the patient on intravenous ceftriaxone 2 g per day and oral acetazolamide 250 mg twice a day. We also continued giving the patient topical levofloxacin 0.5% eye drops, one drop every four hours on the right eye. On the fourth hospital day, the combination of topical and intravenous antibiotics, and acetazolamide offered partial relief of the eye pain but did not improve the conjunctival injection and mucoid discharge.We opted not to do a pars plana vitrectomy due to the fulminant course of the disease. We opened the possibility of enucleation to the patient, depending on the progress of the infection, however the patient was not open to the procedure.
On the fifth day of admission, results of the vitreous fluid culture done on the day of admission showed growth of Klebsiella pneumoniae. There was no growth in the blood culture, but the urine culture also displayed growth of Klebsiella pneumoniae and Staphylococcus. We then started the patient on intravenous gentamicin 80 mg twice a day and continued the medications that we started on the first day.
Given a diabetic patient with a history of complicated UTI a month prior to admission, with minimal flank pain despite antibiotic treatment, and with urine culture findings of Klebsiella pneumoniae during the present admission, we suspected that the patient had persistent renal infection. This underlying infection could also be a possible endogenous source of the patient’s ongoing endophthalmitis.
Therefore, we requested an ultrasound of the whole abdomen, which revealed a left perinephric abscess formation. At this point, we just continued the patient’s ongoing antibiotic treatment. By this time, we were already considering that the etiology of the patient’s endophthalmitis was endogenous.
On the 14th hospital day, the patient complained of worsening left flank pain. We did a contrast CT scan of the whole abdomen which revealed bilateral pyelonephritis with left perinephric and left psoas abscesses (Figure 4). Approximately, 135 mL of fluid collection was visualized in the left psoas muscle region. The Interventional Radiology service performed a CT-guided percutaneous drainage using a pigtail catheter to drain the psoas and perinephric abscesses.
One month after admission, the patient’s eye became phthisical. After five weeks of antibiotic treatment, the pain and swelling on the patient’s right eye resolved, but vision was not restored. A repeat abdominal CT scan done prior to discharge revealed a markedly regressing left psoas and perinephric abscesses (Figure 5). We discharged the patient 41 days after admission. Our final diagnoses for the patient’s conditions were panophthalmitis of the right eye, and resolved perinephric and psoas abscess.
 |
|
Figure 1 Erythematous, edematous, and proptotic right eye of the patient. |

|
|
Figure 2 Anterior segment photo showing diffuse conjunctival injection and extensive fibrin formation in the right eye. |
|
|
Figure 3 B-scan of the right eye, revealing mild- to moderate-amplitude point echoes with choroidal thickening. |

|
|
Figure 4 Coronal (A) and axial (B) views of contrast CT scan of the whole abdomen, done on the 21st hospital day, showing left perinephric and psoas abscesses. |

|
|
Figure 5 Anterior segment photo of the right eye showing marked decrease in anterior chamber inflammation with 360o posterior synechiae. |

|
|
Figure 6 Repeat CT scan on the 40th hospital day showing markedly regressing left psoas and perinephric abscesses. |
Patient consent
Obtained
Reporting guideline used
Article source
Submitted
Peer review
External
Competing interests
None declared
Access and license
This is an Open Access article licensed under the Creative Commons Attribution-NonCommercial 4.0 International License, which allows others to share and adapt the work, provided that derivative works bear appropriate citation to this original work and are not used for commercial purposes. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc/4.0/
References
1. Egan, DJ. Endophthalmitis. 2018 Jul 2 [cited 2020 Jun 29]. In: Medscape. New York: Medscape. C1994-2020. Available from: https://emedicine.medscape.com/article/799431-overview#a6
2. Sheu SJ. Endophthalmitis. Korean J Ophthalmol. 2017 Aug;31(4):283-289. doi: 10.3341/kjo.2017.0036. Epub 2017 Jun 28.
3. Chen KJ, Chen YP, Chao AN, Wang NK, Wu WC, Lai CC, Chen TL. Prevention of evisceration or enucleation in endogenous bacterial panophthalmitis with no light perception and scleral abscess. 2017 PLoS ONE, 12 (1) , art. no. 0169603.
4. Chaudhry IA, Al-Dhibi H, Al-Rashed W, Al- Mezaine HS, Arat YO, Abdelghani W. Endophthalmitis: Experience from a Tertiary Eye Care Center, Common Eye Infections, Imtiaz A. Chaudhry, (May 8th 2013). IntechOpen, DOI: 10.5772/54431. Available from: https://www.intechopen.com/books/common-eye-infections/endophthalmitis-experience-from-a-tertiary-eye-care-center.
5. Durand ML. Bacterial and Fungal Endophthalmitis. Clin Microbiol Rev. 2017 Jul;30(3):597-613. doi: 10.1128/CMR.00113-16.
6. Sadiq MA, Hassan M, Agarwal A, Sarwar S, Toufeeq S, Soliman MK, Hanout M, Sepah YJ, Do DV, Nguyen QD. Endogenous endophthalmitis: diagnosis, management, and prognosis. J Ophthalmic Inflamm Infect. 2015 Dec;5(1):32.
7. Yuan, Z, Liang X, Zhong, J. The disease course of bilateral endogenous fungal endophthalmitis. J Clin Exp Ophthalmol. 2017;8(1):639.
8. Kashani AH, Eliott D. The emergence of Klebsiella pneumoniae endogenous endophthalmitis in the USA: basic and clinical advances. J Ophthalmic Inflamm Infect. 2013;3(1):28. Published 2013 Feb 4.
9. Sridhar J, Flynn HW Jr, Kuriyan AE, Dubovy S, Miller D. Endophthalmitis caused by Klebsiella species. Retina. 2014 Sep;34(9):1875-81.
10. Sheu SJ, Kung YH, Wu TT, Chang FP, Horng YH. Risk factors for endogenous endophthalmitis secondary to klebsiella pneumoniae liver abscess: 20-year experience in Southern Taiwan. Retina. 2011 Nov;31(10):2026-31.
11. Kernt M, Kampik A. Endophthalmitis: Pathogenesis, clinical presentation, management, and perspectives. Clin Ophthalmol. 2010 Mar 24;4:121-35.
12. Davis JL. Diagnostic dilemmas in retinitis and endophthalmitis. Eye (Lond). 2012 Feb;26(2):194-201. doi: 10.1038/eye.2011.299. Epub 2011 Nov 25.
13. Behlau I. Endophthalmitis. Infectious Disease Advisor [Internet]. c2020 [cited 2020 June 30]. Available from: https://www.infectiousdiseaseadvisor.com/home/decision-support-in-medicine/infectious-diseases/endophthalmitis/.
14. Birnbaum, F, Gupta, G. Endogenous endophthalmitis: Diagnosis and treatment. 2016 Jun [cited 2020 June 30]. In: American Academy of Ophthalmology. California: American Academy of Ophthalmology. C2020. Available from: https://www.aao.org/eyenet/article/endogenous-endophthalmitis-diagnosis-treatment.
15. Zhang YQ, Wang WJ. Treatment outcomes after pars plana vitrectomy for endogenous endophthalmitis. Retina. 2005 Sep;25(6):746-50.
16. Vaziri K, Schwartz SG, Kishor K, Flynn HW Jr. Endophthalmitis: state of the art. Clin Ophthalmol. 2015 Jan 8;9:95-108.
17. Yonekawa Y, Chan RP, Reddy AK, Pieroni CG, Lee TC, & Lee S. Early intravitreal treatment of endogenous bacterial endophthalmitis. Clinical & Experimental Ophthalmology. 2011 39(8), 771–778.
18. Peyman GA, Raichand M, Bennett TO. Management of endophthalmitis with pars plana vitrectomy. Br J Ophthalmol. 1980 Jul;64(7):472-5.
Copyright © 2020 CGP Malabanan, et al.

Published
June 30, 2020
Issue
Volume 6 Issue 1 (2020)
Section
Case in images

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Authors who publish with this journal agree to the following terms:
- Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution-NonCommercial 4.0 International License that allows others to share the work for non-commercial purposes with an acknowledgement of the work's authorship and initial publication in this journal.
- Authors are able to enter into separate, additional, non-commercial contractual arrangements for the non-exclusive distribution of the journal's published version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgement of its initial publication in this journal.
- Authors grant the journal permission to rewrite, edit, modify, store and/or publish the submission in any medium or format a version or abstract forming part thereof, all associated supplemental materials, and subsequent errata, if necessary, in a publicly available publication or database.
- Authors warrant that the submission is original with the authors and does not infringe or transfer any copyright or violate any other right of any third parties.